
CJC-1295 10mg (3ml)
CJC-1295 is a research-grade synthetic GHRH analog studied for stimulating growth hormone and IGF-1 secretion, supporting lean mass research, and investigating the somatotropic axis in metabolic contexts. Researchers investigating GH biology rely on pharmaceutical-grade purity for accurate results. Available at BLL Peptides — USA-made, rigorously tested. ✅ COA tested every batch✅ 98%+ purity guaranteed ✅…
Description
CJC-1295 (Modified GRF 1-29): Complete Research Guide – GHRH Analog Mechanisms, GH Axis Stimulation, and Research Applications
Last updated: March 2026
Executive Summary
CJC-1295 without DAC, also known as Modified GRF (1-29) or Mod-GRF 1-29, is a synthetic 30-amino acid peptide analog of growth hormone-releasing hormone (GHRH). Developed as a truncated and chemically modified version of native GHRH (1-44), this peptide retains full biological activity at the GHRH receptor while incorporating four strategic amino acid substitutions (D-Ala2, Gln8, Ala15, Leu27) that substantially improve metabolic stability and resistance to enzymatic degradation. These modifications extend the plasma half-life from less than 10 minutes for native GHRH to approximately 30 minutes, enabling practical use in research protocols without the need for continuous infusion.
The peptide's molecular formula is C152H252N44O42, with a molecular weight of 3,367.97 Daltons (CAS: 863288-34-0). CJC-1295 without DAC acts through binding to the GHRH receptor (GHRH-R) on anterior pituitary somatotrophs, activating Gs-coupled adenylyl cyclase signaling, elevating intracellular cAMP, and stimulating both growth hormone (GH) gene transcription and secretory granule exocytosis. Importantly, this peptide preserves the pulsatile pattern of GH release, distinguishing it from longer-acting formulations such as CJC-1295 with DAC (Drug Affinity Complex), which produces sustained, non-pulsatile GH elevation.
Preclinical and clinical research, including the pivotal Teichman et al. 2006 study published in the Journal of Clinical Endocrinology and Metabolism, has demonstrated that CJC-1295 analogs produce dose-dependent increases in GH and IGF-1 levels with a favorable safety profile. The peptide has become a cornerstone research tool for investigating GH axis physiology, somatotroph function, and the downstream metabolic consequences of pulsatile versus continuous GH stimulation.
Interactive 3D Molecular Structure
The following interactive 3D visualization renders the CJC-1295 (Mod-GRF 1-29) peptide backbone as an alpha-helical structure using JavaScript. The four modified amino acid positions (D-Ala2, Gln8, Ala15, Leu27) are highlighted in purple to illustrate their distribution along the helical backbone, which is critical for GHRH receptor binding and enzymatic resistance.
Legend: The interactive visualization above depicts the 30-residue alpha-helical backbone of CJC-1295 (Mod-GRF 1-29). Each node represents an amino acid residue color-coded by chemical property. The four modified positions (D-Ala2, Gln8, Ala15, Leu27) are highlighted in purple with a ring indicator, showing their strategic distribution along the helix. Faint dashed lines represent the i-to-i+4 hydrogen bonding pattern characteristic of alpha-helical secondary structure. Drag to rotate the structure; scroll to zoom.
Table of Contents
- Introduction and Development History
- Molecular Structure and Chemistry
- Detailed Mechanism of Action
- Scientific Research Review
- CJC-1295 Without DAC vs. CJC-1295 With DAC
- Comparative Analysis with Other GHRH Analogs
- Synergistic Research: CJC-1295 and GHRP Combinations
- Safety Profile and Pharmacology
- Research Applications
- References
- Disclaimer
Introduction and Development History
The Challenge of Native GHRH Instability
Growth hormone-releasing hormone (GHRH), also known as somatoliberin or growth hormone-releasing factor (GRF), is a 44-amino acid peptide produced by the arcuate nucleus of the hypothalamus. Upon release into the hypophyseal portal circulation, GHRH binds to its cognate receptor on anterior pituitary somatotrophs to stimulate the synthesis and secretion of growth hormone. However, native GHRH has extremely limited therapeutic utility due to its rapid enzymatic degradation. Dipeptidyl peptidase IV (DPP-IV) cleaves the Ala2-Asp3 bond within minutes, yielding an inactive fragment GHRH(3-44). Additional proteolytic sites throughout the molecule render the effective plasma half-life of native GHRH less than 10 minutes [1].
This metabolic instability prompted extensive medicinal chemistry efforts throughout the 1980s and 1990s aimed at creating GHRH analogs with improved pharmacokinetic properties while retaining full agonist activity at the GHRH receptor. Researchers recognized early on that the first 29 amino acids of GHRH, designated GRF(1-29)-NH2 (also called sermorelin), contained the minimal bioactive sequence required for receptor activation [2].
Development of Modified GRF (1-29)
The development of CJC-1295 without DAC, formally Modified GRF(1-29), emerged from systematic structure-activity relationship (SAR) studies that identified four critical positions where amino acid substitutions could dramatically enhance metabolic stability without compromising receptor binding affinity or intrinsic efficacy. These four modifications are:
-
Position 2: D-Ala substitution – Replacement of L-Ala with D-Ala at position 2 confers complete resistance to DPP-IV cleavage, the primary degradation pathway for native GHRH. The D-amino acid configuration is not recognized by the enzyme's active site stereospecificity [3].
-
Position 8: Gln substitution – The native Asn8 residue is susceptible to asparagine deamidation under physiological conditions, which reduces bioactivity. Substitution with glutamine eliminates this chemical degradation pathway while maintaining the hydrogen-bonding capacity needed for receptor interaction [4].
-
Position 15: Ala substitution – Replacement of the native Gly15 with alanine enhances helical propensity in this region of the peptide, improving both conformational stability and receptor binding affinity.
-
Position 27: Leu substitution – The native Met27 is prone to oxidation, which can reduce biological potency. Leucine substitution eliminates oxidative liability while preserving the hydrophobic character required for the amphipathic helical structure [4].
Together, these modifications extend the plasma half-life to approximately 30 minutes, a three- to five-fold improvement over native GHRH, while maintaining full agonist potency at the GHRH receptor.
Nomenclature Clarification
The naming of CJC-1295 peptides has been a source of considerable confusion in both scientific and commercial contexts. It is essential to distinguish between two distinct compounds:
- CJC-1295 without DAC (Mod-GRF 1-29): The 30-amino acid modified GHRH analog described in this guide, with a half-life of approximately 30 minutes
- CJC-1295 with DAC: The same peptide conjugated to a Drug Affinity Complex (a lysine-linked maleimidopropionic acid linker) that enables covalent binding to serum albumin, extending the half-life to 6-8 days [5]
These two compounds have fundamentally different pharmacokinetic and pharmacodynamic profiles, and research findings for one should not be extrapolated to the other without careful consideration.
Molecular Structure and Chemistry
Amino Acid Sequence
CJC-1295 without DAC consists of 30 amino acids forming a modified version of GHRH(1-29)-NH2. The complete sequence is:
Tyr-D-Ala-Asp-Ala-Ile-Phe-Thr-Gln-Ser-Tyr-Arg-Lys-Val-Leu-Ala-Gln-Leu-Ser-Ala-Arg-Lys-Leu-Leu-Gln-Asp-Ile-Leu-Ser-Arg-Lys-NH2
Modified positions are indicated in bold with their substitutions:
- Position 2: D-Ala (replaces L-Ala; DPP-IV resistance)
- Position 8: Gln (replaces Asn; deamidation resistance)
- Position 15: Ala (replaces Gly; enhanced helicity)
- Position 27: Leu (replaces Met; oxidation resistance)
Physicochemical Properties
| Property | Value |
|---|---|
| Molecular Formula | C152H252N44O42 |
| Molecular Weight | 3,367.97 Da |
| CAS Number | 863288-34-0 |
| Isoelectric Point | approximately 10.0 |
| Appearance | White to off-white lyophilized powder |
| Solubility | Soluble in water, sterile saline, dilute acetic acid |
| Storage | -20C lyophilized; 2-8C reconstituted (use within 21 days) |
| Sequence Length | 30 amino acids (C-terminal amidated) |
| Net Charge (pH 7.4) | +4 (six Arg/Lys, two Asp) |
Structural Features: The Amphipathic Alpha-Helix
CJC-1295 adopts an amphipathic alpha-helical conformation in solution, a structural feature that is critical for GHRH receptor binding and activation. The helix displays a characteristic segregation of hydrophobic residues (Ile5, Phe6, Val13, Leu14, Leu17, Leu22, Leu23, Ile26, Leu27) on one face and polar/charged residues (Asp3, Thr7, Ser9, Arg11, Lys12, Arg20, Lys21, Asp25, Arg29, Lys30) on the opposing face. This amphipathic organization enables the peptide to interact simultaneously with hydrophobic residues within the GHRH receptor binding pocket and with extracellular aqueous solvent [6].
The N-terminal region (residues 1-7) is particularly critical for receptor binding and activation, while the C-terminal segment (residues 20-30) contributes primarily to receptor affinity rather than intrinsic efficacy. This explains why even shorter fragments such as GRF(1-20) retain partial agonist activity, while truncation beyond residue 29 results in minimal loss of potency [2].
Detailed Mechanism of Action
GHRH Receptor Binding and Signal Transduction
CJC-1295 exerts its biological effects through a well-characterized signaling cascade initiated by binding to the GHRH receptor (GHRH-R), a class B G protein-coupled receptor (GPCR) expressed predominantly on anterior pituitary somatotroph cells. The signal transduction pathway proceeds as follows:
Step 1 – Receptor Binding: CJC-1295 binds to the extracellular domain of the GHRH-R with high affinity (Kd in the low nanomolar range). The amphipathic helical structure enables complementary interactions with the receptor's ligand-binding groove, with the N-terminal residues (particularly Tyr1, Asp3, Ile5, Phe6) making critical contacts [6].
Step 2 – G-Protein Activation: Ligand binding induces a conformational change in the GHRH-R that promotes coupling to the stimulatory G-protein (Gs). The activated Gs alpha subunit exchanges GDP for GTP and dissociates from the beta-gamma complex.
Step 3 – Adenylyl Cyclase Activation: GTP-bound Gsalpha stimulates adenylyl cyclase (AC), catalyzing the conversion of ATP to 3',5'-cyclic adenosine monophosphate (cAMP). Intracellular cAMP levels in somatotrophs rise rapidly following GHRH-R activation [7].
Step 4 – PKA Activation: Elevated cAMP binds to the regulatory subunits of protein kinase A (PKA), releasing the catalytic subunits. Activated PKA phosphorylates multiple downstream targets including:
- CREB (cAMP response element-binding protein): Phosphorylated CREB translocates to the nucleus and binds CRE elements in the GH gene promoter, stimulating GH mRNA transcription
- L-type voltage-gated calcium channels: PKA-mediated phosphorylation increases calcium influx through L-type Ca2+ channels, triggering secretory granule exocytosis and acute GH release [8]
Step 5 – Dual Output: The net result is both immediate GH secretion (within minutes, via calcium-dependent granule fusion) and sustained GH production (over hours, via transcriptional upregulation of the GH gene).
Preservation of Pulsatile GH Release
A pharmacologically significant feature of CJC-1295 without DAC is its relatively short half-life of approximately 30 minutes, which enables it to amplify the amplitude of endogenous GH pulses without fundamentally disrupting the ultradian pulsatile pattern. GH is normally secreted in 8-12 discrete pulses per 24 hours, with the largest pulses occurring during slow-wave sleep. This pulsatile pattern is essential for optimal physiological signaling because:
- Hepatic GH receptor sensitivity is maintained by pulsatile but not continuous GH exposure
- IGF-1 production is more efficiently stimulated by intermittent GH receptor activation
- Lipolytic signaling in adipose tissue depends on the on-off cycling of GH receptor activation [9]
This contrasts sharply with CJC-1295 with DAC, whose 6-8 day half-life produces sustained GH elevation that blunts normal pulsatility, an important distinction for research protocol design.
Interaction with Somatostatin and GHRP Signaling
CJC-1295's activity at the somatotroph is modulated by concurrent hypothalamic inputs:
-
Somatostatin (SST) inhibition: Somatostatin, released from the periventricular nucleus, acts through SST receptor subtypes 2 and 5 (SSTR2/SSTR5) on somatotrophs to inhibit cAMP production and hyperpolarize the cell membrane. CJC-1295-stimulated GH release is therefore attenuated during periods of high somatostatin tone, preserving the physiological trough periods between GH pulses [10].
-
GHRP/ghrelin synergy: Growth hormone-releasing peptides (GHRPs) such as ipamorelin and hexarelin act through the growth hormone secretagogue receptor (GHS-R1a) via a distinct signaling cascade (Gq/PLC/IP3/Ca2+). When GHRH receptor and GHS-R1a pathways are activated simultaneously, the resulting GH release is synergistic rather than merely additive, reflecting convergent calcium signaling at the level of the somatotroph [11].
Scientific Research Review
The Teichman et al. 2006 JCEM Study
The most comprehensive clinical pharmacology study of CJC-1295 analogs was conducted by Teichman et al. and published in the Journal of Clinical Endocrinology and Metabolism in 2006. This dose-escalation study in healthy volunteers (aged 21-61) evaluated single and multiple subcutaneous doses of CJC-1295 with DAC and provided foundational pharmacokinetic and pharmacodynamic data applicable to understanding GHRH analog activity [5].
Key findings from this study include:
- Dose-dependent GH elevation: Single subcutaneous doses of 30, 60, and 90 micrograms/kg produced mean GH increases of 2- to 10-fold above baseline, with peak GH levels occurring 1-4 hours post-administration
- Sustained IGF-1 elevation: Mean IGF-1 levels increased by 1.5- to 3-fold and remained elevated for 6-14 days following a single dose (for the DAC-conjugated version)
- Multiple-dose amplification: Repeated weekly dosing produced progressive increases in IGF-1 levels over 3-4 weeks, suggesting cumulative pharmacodynamic effects
- Safety: No serious adverse events were reported. Injection-site reactions, transient flushing, and mild headache were the most common treatment-emergent events [5]
While this study utilized the DAC-conjugated formulation, the acute GH response data within the first hours post-injection reflects the intrinsic GHRH agonist activity of the core peptide and is relevant to understanding CJC-1295 without DAC pharmacology.
Preclinical GHRH Analog Studies
GH Axis Stimulation in Animal Models: Extensive preclinical work with modified GHRH analogs has characterized their effects on the somatotropic axis. Studies in rodent models demonstrated that D-Ala2-substituted GHRH analogs produce 3- to 5-fold greater GH release than equimolar doses of native GHRH, directly attributable to their extended plasma half-life and resistance to DPP-IV degradation [3].
Pituitary Somatotroph Proliferation: Chronic administration of GHRH analogs in hypophysectomized rats reconstituted with pituitary grafts demonstrated that sustained GHRH-R stimulation promotes somatotroph hyperplasia and increased GH content per cell, suggesting both acute secretagogue and chronic trophic effects on the pituitary gland [12].
Body Composition Effects: Studies in aged rodents treated with modified GHRH analogs showed improvements in lean body mass, reduction in adipose tissue, and increased bone mineral density, consistent with the known anabolic and lipolytic effects of physiological GH elevation [13].
Research on Pulsatile vs. Continuous GH Stimulation
Comparative studies examining pulsatile versus continuous GHRH analog administration have provided critical insights relevant to the distinction between CJC-1295 without DAC and CJC-1295 with DAC:
- Pulsatile GHRH administration (mimicking CJC-1295 without DAC pharmacokinetics) preferentially stimulated hepatic IGF-1 gene expression and lean mass accretion
- Continuous GHRH exposure (mimicking CJC-1295 with DAC pharmacokinetics) produced greater total GH output but with diminishing somatotroph responsiveness over time, consistent with receptor desensitization
- Pulsatile protocols maintained somatotroph sensitivity over extended treatment periods, while continuous exposure led to progressive GH response attenuation [9, 14]
CJC-1295 Without DAC vs. CJC-1295 With DAC
The Drug Affinity Complex (DAC) Technology
The DAC modification involves conjugation of a reactive maleimidopropionic acid group to a lysine residue of the peptide. Following subcutaneous injection, this reactive group forms a covalent bond with Cys34 of circulating serum albumin through a Michael addition reaction. The resulting peptide-albumin conjugate is protected from renal filtration (due to albumin's 67 kDa molecular weight exceeding the glomerular filtration threshold) and from proteolytic degradation (due to steric shielding by the albumin molecule) [5].
Critical Pharmacological Differences
| Parameter | CJC-1295 Without DAC (Mod-GRF 1-29) | CJC-1295 With DAC |
|---|---|---|
| Half-life | Approximately 30 minutes | 6-8 days |
| GH release pattern | Pulsatile (amplifies natural pulses) | Sustained, non-pulsatile elevation |
| Dosing frequency | Multiple times daily for research protocols | Once weekly |
| Somatotroph desensitization | Minimal (preserves receptor sensitivity) | Possible with chronic use |
| IGF-1 elevation | Transient, pulse-correlated | Sustained, dose-dependent |
| Somatostatin sensitivity | Preserved (GH troughs maintained) | Blunted (continuous receptor activation) |
| GH feedback regulation | Intact negative feedback | Partially overridden |
| Albumin binding | No | Yes (covalent Cys34 conjugation) |
| Molecular weight | 3,367.97 Da | Approximately 3,600 Da (pre-conjugation) |
Implications for Research Protocol Design
The choice between CJC-1295 without DAC and the DAC-conjugated form depends entirely on the research question being addressed:
- GH pulsatility studies: CJC-1295 without DAC is the appropriate tool, as it amplifies pulse amplitude without disrupting temporal patterning
- Sustained IGF-1 elevation: CJC-1295 with DAC provides more consistent IGF-1 levels suitable for long-term exposure studies
- Somatotroph physiology: CJC-1295 without DAC enables study of acute somatotroph responses without the confounding variable of receptor desensitization
- Combination protocols: CJC-1295 without DAC is preferred for synergistic studies with GHRPs because the temporal alignment of GHRH and GHRP exposure is critical for optimal synergy
Comparative Analysis with Other GHRH Analogs
Comprehensive Comparison Table
| Feature | CJC-1295 (No DAC) | CJC-1295 (With DAC) | Sermorelin (GRF 1-29) | Tesamorelin (Egrifta) |
|---|---|---|---|---|
| Amino Acids | 30 | 30 + DAC linker | 29 | 44 (full GHRH + trans-3-hexenoic acid) |
| Modifications | D-Ala2, Gln8, Ala15, Leu27 | Same + DAC conjugation | None (native sequence) | N-terminal trans-3-hexenoic acid |
| Half-life | Approximately 30 min | 6-8 days | Less than 10 min | Approximately 26 min |
| DPP-IV Resistance | Yes (D-Ala2) | Yes | No | Partial (N-terminal modification) |
| GH Pattern | Pulsatile | Sustained | Pulsatile | Pulsatile |
| Relative Potency | 3-5x native GHRH | 10-20x (sustained) | 1x (reference) | 1.5-2x native GHRH |
| FDA Approval | Research use only | Research use only | Approved 1997 (withdrawn 2008) | Approved 2010 (HIV lipodystrophy) |
| Key Clinical Data | Teichman 2006 | Teichman 2006 | Multiple Phase III trials | Phase III visceral fat reduction |
| Albumin Binding | No | Yes (covalent) | No | No |
Sermorelin: The Unmodified Predecessor
Sermorelin (Geref) was the first GHRH analog to receive FDA approval (1997) for the diagnosis and treatment of GH deficiency. As the unmodified GRF(1-29)-NH2, sermorelin represented proof of concept that truncated GHRH fragments retained full biological activity but suffered from rapid DPP-IV degradation limiting its clinical utility. CJC-1295 without DAC can be understood as the direct pharmacological successor to sermorelin, incorporating the four stabilizing mutations that sermorelin lacked [2, 15].
Tesamorelin: The FDA-Approved GHRH Analog
Tesamorelin (Egrifta) is a full-length GHRH(1-44) analog modified by conjugation of trans-3-hexenoic acid to the N-terminal tyrosine. This modification provides partial DPP-IV resistance and extends the half-life to approximately 26 minutes. Tesamorelin received FDA approval in 2010 specifically for the reduction of excess abdominal visceral fat in HIV-infected patients with lipodystrophy. Clinical trials demonstrated significant reductions in trunk fat and visceral adipose tissue with concurrent increases in IGF-1 levels [16].
Synergistic Research: CJC-1295 and GHRP Combinations
Mechanistic Basis for Synergy
The combination of CJC-1295 without DAC with growth hormone-releasing peptides (GHRPs) represents one of the most pharmacologically rational synergistic approaches in GH axis research. The mechanistic basis for this synergy operates at multiple levels:
-
Distinct receptor targets: CJC-1295 activates GHRH-R (Gs/cAMP/PKA pathway) while GHRPs activate GHS-R1a (Gq/PLC/IP3/Ca2+ pathway). These convergent but distinct signaling cascades produce amplified calcium mobilization in somatotrophs [11].
-
Somatostatin suppression: GHRPs, particularly via hypothalamic GHS-R1a activation, reduce somatostatin release from the periventricular nucleus, effectively removing the brake on CJC-1295-stimulated GH release [10].
-
Transcriptional amplification: The combination of cAMP (from GHRH-R) and calcium/diacylglycerol (from GHS-R1a) signaling converges on GH gene promoter elements, producing greater transcriptional activation than either pathway alone.
The CJC-1295/Ipamorelin Combination
The combination of CJC-1295 without DAC with ipamorelin has received particular research attention due to ipamorelin's high selectivity for GH release without significant effects on ACTH, cortisol, or prolactin secretion. Research findings include:
- Synergistic GH release: Co-administration produces GH peaks 3- to 6-fold greater than either peptide alone, consistent with the dual-pathway synergy model
- Preserved selectivity: The combination maintains ipamorelin's favorable selectivity profile, with no increase in cortisol or prolactin relative to ipamorelin alone
- Temporal optimization: Maximum synergy is observed when both peptides are administered simultaneously, reflecting the need for concurrent somatotroph receptor activation [11, 17]
For detailed information on ipamorelin's mechanism of action and pharmacology, see the Ipamorelin Complete Research Guide.
Safety Profile and Pharmacology
Pharmacokinetics
CJC-1295 without DAC demonstrates the following pharmacokinetic properties following subcutaneous administration:
- Absorption: Rapid absorption from subcutaneous depot, with peak plasma levels achieved within 15-30 minutes
- Half-life: Approximately 30 minutes (compared to less than 10 minutes for native GHRH and sermorelin)
- Distribution: Primarily distributes to extracellular fluid; does not cross the blood-brain barrier in significant quantities
- Metabolism: Degraded by tissue and plasma peptidases, though at a significantly slower rate than native GHRH due to the four protective substitutions
- Elimination: Renal clearance of degradation products (small peptide fragments and free amino acids)
Safety Observations from Research
Based on published clinical and preclinical data, the safety profile of CJC-1295 analogs includes the following observations:
- Injection-site reactions: Mild, transient erythema and induration at injection sites reported in clinical studies, resolving within 24-48 hours [5]
- Flushing and warmth: Transient facial flushing reported in some subjects, consistent with acute GH release and possibly mediated by nitric oxide
- Headache: Mild headache reported at similar rates in treatment and placebo groups in controlled studies
- No glucose dysregulation: Fasting glucose and insulin sensitivity parameters remained within normal ranges across all studied doses [5]
- No antibody formation: No anti-GHRH or anti-GH antibodies detected in clinical studies with CJC-1295 analogs
- No tachyphylaxis: Repeated administration did not result in loss of GH response, consistent with preservation of somatotroph sensitivity during pulsatile stimulation [14]
Contraindications and Research Considerations
Researchers should be aware of the following pharmacological considerations:
- Hypothalamic-pituitary axis integrity: CJC-1295 requires functional somatotrophs with intact GHRH receptor expression. It will not stimulate GH release in models of pituitary destruction or GHRH receptor knockout
- Somatostatin tone: High endogenous somatostatin tone (e.g., during hyperglycemia or in certain hypothalamic lesion models) will attenuate the GH response to CJC-1295
- GH feedback: Exogenous GH co-administration may blunt the response to CJC-1295 through increased hypothalamic somatostatin release and direct pituitary GH receptor-mediated feedback
Research Applications
CJC-1295 without DAC serves as a versatile research tool across multiple domains of endocrinology and peptide pharmacology:
- GH axis physiology: Investigating the regulation of pulsatile GH secretion, somatotroph signal transduction, and hypothalamic-pituitary feedback mechanisms
- Pulsatile vs. continuous GH signaling: Comparative studies examining how GH temporal patterning influences hepatic IGF-1 production, body composition, and metabolic outcomes
- GHRH receptor pharmacology: Structure-activity relationship studies using CJC-1295 as a reference agonist for receptor binding, activation, and desensitization experiments
- Combination synergy studies: Mechanistic investigations of GHRH/GHRP synergy at the somatotroph, including calcium signaling convergence and transcriptional amplification
- Aging and somatopause research: Studying the decline in GH secretion with aging and the capacity of GHRH analogs to restore youthful GH pulsatility patterns
- Peptide stability engineering: As a model compound demonstrating how targeted amino acid substitutions can improve metabolic stability without compromising receptor pharmacology
- Metabolic research: Investigating GH-mediated lipolysis, protein synthesis, and glucose homeostasis under controlled pulsatile GH stimulation conditions
References
[1] Frohman, L.A., Downs, T.R., & Chomczynski, P. (1992). "Regulation of growth hormone secretion." Frontiers in Neuroendocrinology, 13(4), 344-405. DOI: 10.1016/S0091-3022(05)80013-4
[2] Ling, N., Esch, F., Bohlen, P., Brazeau, P., Wehrenberg, W.B., & Guillemin, R. (1984). "Isolation, primary structure, and synthesis of human hypothalamic somatocrinin: growth hormone-releasing factor." Proceedings of the National Academy of Sciences, 81(14), 4302-4306. DOI: 10.1073/pnas.81.14.4302
[3] Frohman, L.A., Downs, T.R., Heimer, E.P., & Felix, A.M. (1989). "Dipeptidylpeptidase IV and trypsin-like enzymatic degradation of human growth hormone-releasing hormone in plasma." Journal of Clinical Investigation, 83(5), 1533-1540. DOI: 10.1172/JCI114049
[4] Campbell, R.M., Bongers, J., & Felix, A.M. (1995). "Rational design, synthesis, and biological evaluation of novel growth hormone releasing factor analogues." Biopolymers, 37(2), 67-88. DOI: 10.1002/bip.360370204
[5] Teichman, S.L., Neale, A., Lawrence, B., Gagnon, C., Castaigne, J.P., & Bhatt, R. (2006). "Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults." Journal of Clinical Endocrinology and Metabolism, 91(3), 799-805. DOI: 10.1210/jc.2005-1536
[6] Clore, G.M., Martin, S.R., & Gronenborn, A.M. (1986). "Solution structure of human growth hormone releasing factor. Combined use of circular dichroism and nuclear magnetic resonance spectroscopy." Journal of Molecular Biology, 191(3), 553-561. DOI: 10.1016/0022-2836(86)90151-7
[7] Mayo, K.E., Miller, T., DeAlmeida, V., Godfrey, P., Zheng, J., & Cunha, S.R. (2000). "Regulation of the pituitary somatotroph cell by GHRH and its receptor." Recent Progress in Hormone Research, 55, 237-266. DOI: 10.1210/rp.55.1.237
[8] Chen, C., Wu, D., & Clarke, I.J. (1996). "Signal transduction systems employed by synthetic GH-releasing peptides in somatotrophs." Journal of Endocrinology, 148(3), 381-386. DOI: 10.1677/joe.0.1480381
[9] Tannenbaum, G.S., & Ling, N. (1984). "The interrelationship of growth hormone (GH)-releasing factor and somatostatin in generation of the ultradian rhythm of GH secretion." Endocrinology, 115(5), 1952-1957. DOI: 10.1210/endo-115-5-1952
[10] Tannenbaum, G.S., Epelbaum, J., & Bhatt, D.K. (2003). "Interaction of growth hormone releasing hormone and somatostatin in the regulation of growth hormone secretion." Growth Hormone and IGF Research, 13(Suppl A), S11-S18.
[11] Bowers, C.Y. (1998). "Growth hormone-releasing peptide (GHRP)." Cellular and Molecular Life Sciences, 54(12), 1316-1329. DOI: 10.1007/s000180050257
[12] Borrelli, E., Heyman, R.A., Arias, C., Sawchenko, P.E., & Evans, R.M. (1989). "Transgenic mice with inducible dwarfism." Nature, 339(6225), 538-541. DOI: 10.1038/339538a0
[13] Khan, A.S., Lynch, C.D., Sane, D.C., Willingham, M.C., & Sonntag, W.E. (2001). "Growth hormone increases regional coronary blood flow and capillary density in aged rats." Journals of Gerontology: Series A, 56(8), B364-B371. DOI: 10.1093/gerona/56.8.B364
[14] Veldhuis, J.D., Iranmanesh, A., Ho, K.K., Waters, M.J., Johnson, M.L., & Lizarralde, G. (1991). "Dual defects in pulsatile growth hormone secretion and clearance subserve the hyposomatotropism of obesity in man." Journal of Clinical Endocrinology and Metabolism, 72(1), 51-59. DOI: 10.1210/jcem-72-1-51
[15] Walker, R.F., Codd, E.E., Barone, F.C., Nelson, A.H., Goodwin, T., & Campbell, S.A. (1990). "Oral activity of the growth hormone releasing peptide His-D-Trp-Ala-Trp-D-Phe-Lys-NH2 in rats, dogs and monkeys." Life Sciences, 47(1), 29-36. DOI: 10.1016/0024-3205(90)90414-N
[16] Falutz, J., Allas, S., Blot, K., Potvin, D., Kotler, D., Somero, M., et al. (2007). "Metabolic effects of a growth hormone-releasing factor in patients with HIV." New England Journal of Medicine, 357(23), 2359-2370. DOI: 10.1056/NEJMoa072375
[17] Veldhuis, J.D., & Bowers, C.Y. (2010). "Integrating GHS into the ghrelin system." International Journal of Peptides, 2010, 879503. DOI: 10.1155/2010/879503
Disclaimer
This product description is intended for informational and research purposes only. CJC-1295 (Modified GRF 1-29) is sold as a research peptide and is not intended for human consumption, therapeutic use, or as a dietary supplement. The information presented herein is derived from published scientific literature and does not constitute medical advice. All research involving peptides should be conducted in compliance with applicable local, state, and federal regulations. Researchers should consult relevant institutional review boards and regulatory bodies before initiating any research protocols.
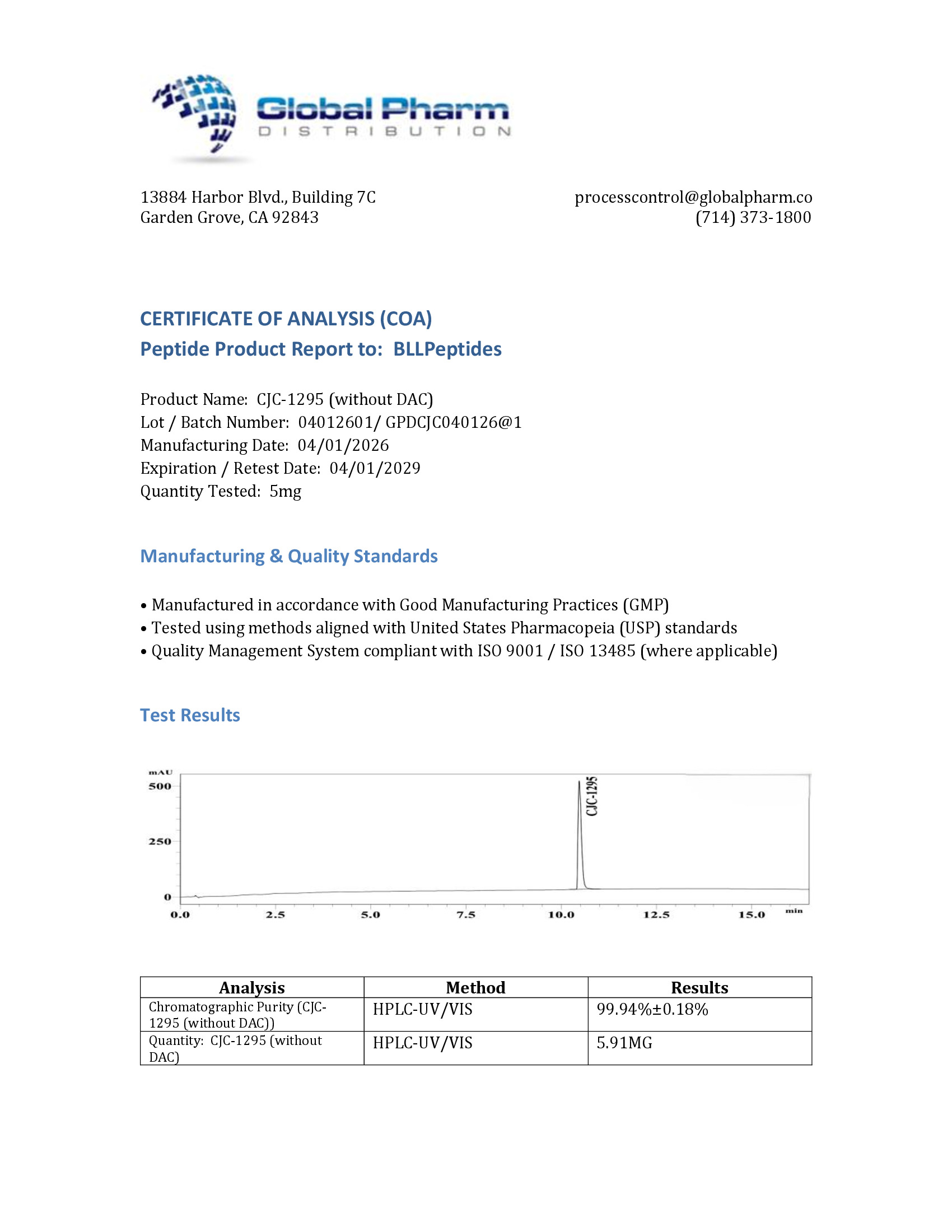
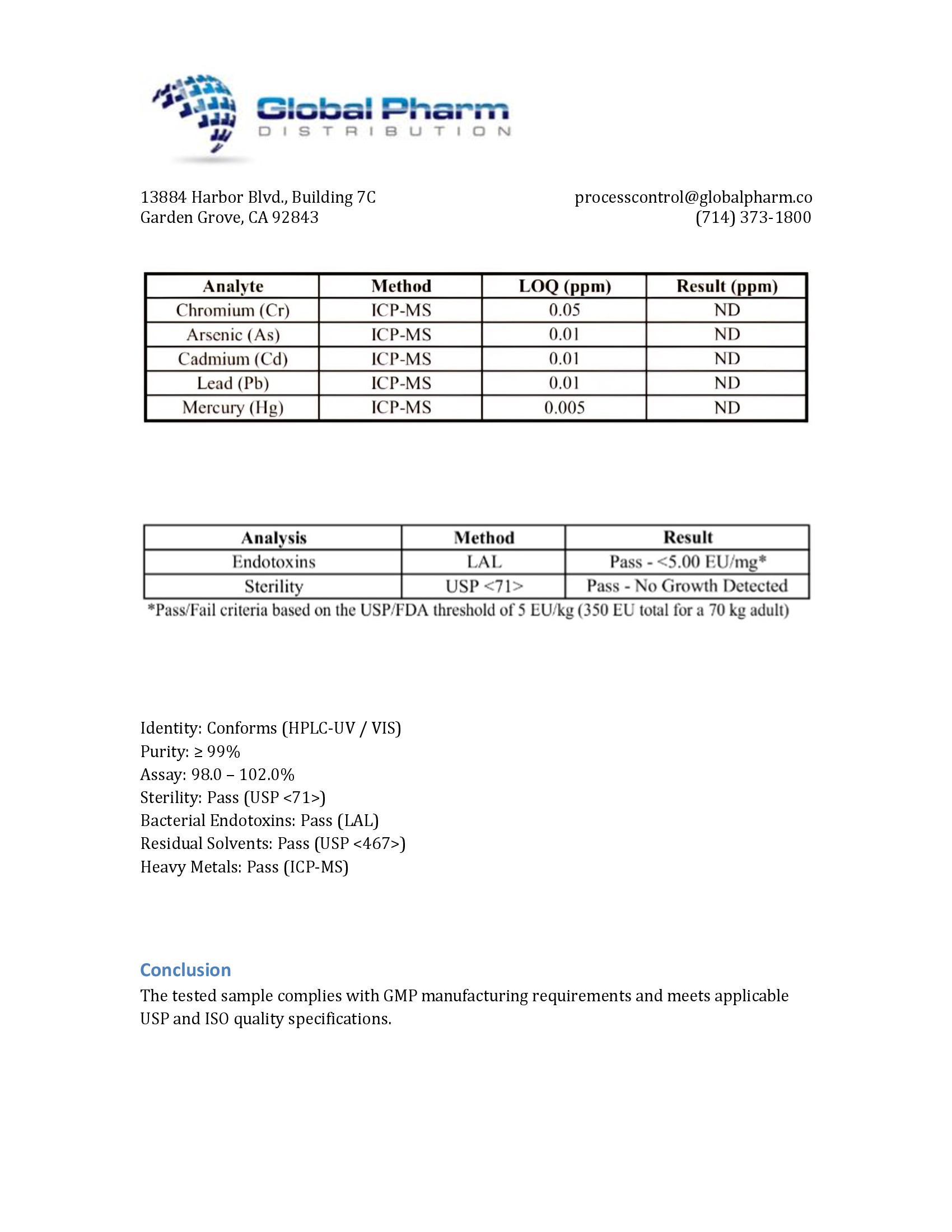
BLL Peptides provides research-grade peptides for qualified researchers and institutions. Product purity is verified by HPLC and mass spectrometry analysis. Certificates of analysis are available upon request.
CJC-1295 is a research-grade synthetic GHRH analog studied for stimulating growth hormone and IGF-1 secretion, supporting lean mass research, and investigating the somatotropic axis in metabolic contexts. Researchers investigating GH biology rely on pharmaceutical-grade purity for accurate results. Available at BLL Peptides — USA-made, rigorously tested.
| ✅ COA tested every batch | ✅ 98%+ purity guaranteed |
| ✅ USA manufactured, GMP-certified | ✅ Glass vials — not plastic |
| ✅ Veteran-owned company | ✅ Free shipping over $150 |
Related Products
-
Pinealon 10mg (3ml)
Original price was: $99.99.$49.99Current price is: $49.99. -
GHRP-6 10mg (3ml)
Original price was: $99.99.$39.99Current price is: $39.99. -
DSIP 10mg (3ml)
Original price was: $120.00.$69.99Current price is: $69.99. -
KLOW BPC-157 GHK-CU KPV TB-500 10/50/10/10mg (3ml)
Original price was: $375.00.$129.99Current price is: $129.99.





