
Ipamorelin 10mg (3ml)
Ipamorelin is a research-grade selective growth hormone secretagogue and ghrelin receptor agonist studied for a clean GH-releasing profile with minimal cortisol and prolactin effects on body composition and recovery. Researchers investigating the GH/IGF-1 axis rely on pharmaceutical-grade purity for reproducible experimental results. Available at BLL Peptides — USA-made, rigorously tested. ✅ COA tested every batch✅…
Description
Ipamorelin: Complete Research Guide – Selective Growth Hormone Secretagogue Mechanisms, Clinical Evidence, and Research Applications
Last updated: March 2026
Executive Summary
Ipamorelin is a synthetic pentapeptide growth hormone secretagogue (GHS) that acts as a selective agonist of the growth hormone secretagogue receptor type 1a (GHS-R1a), also known as the ghrelin receptor. Developed by Novo Nordisk in the late 1990s, ipamorelin is distinguished from all other growth hormone-releasing peptides (GHRPs) by its remarkable selectivity: it stimulates growth hormone (GH) release from the anterior pituitary without affecting serum levels of cortisol, prolactin, adrenocorticotropic hormone (ACTH), or aldosterone at GH-effective doses. This selectivity profile is unmatched among peptidyl GH secretagogues and positions ipamorelin as a uniquely clean pharmacological tool for GH axis research.
The peptide's amino acid sequence is Aib-His-D-2-Nal-D-Phe-Lys-NH2, incorporating three non-natural amino acid residues that confer metabolic stability and receptor selectivity. Its molecular formula is C38H49N9O5, with a molecular weight of 711.85 Daltons (CAS: 170851-70-4). Unlike GHRP-6 and GHRP-2, which stimulate appetite through ghrelin-mimetic activity and elevate cortisol and prolactin at effective doses, ipamorelin produces a dose-dependent, GH-specific secretory response that closely mirrors the physiological pulsatile pattern of natural GH release.
Ipamorelin's mechanism of action involves binding to GHS-R1a on somatotroph cells of the anterior pituitary, activating Gq/11-coupled signaling through phospholipase C (PLC), generating inositol trisphosphate (IP3) and diacylglycerol (DAG), and ultimately triggering calcium-dependent GH vesicle exocytosis. Clinical investigation by Helsinn Healthcare in Phase II trials for post-operative ileus demonstrated both the efficacy and safety of the compound in human subjects. Additional preclinical research has revealed significant effects on bone mineral density and body composition, expanding ipamorelin's research utility beyond neuroendocrine pharmacology into musculoskeletal and metabolic domains.
Interactive 3D Molecular Structure
The following interactive 3D visualization renders the ipamorelin pentapeptide in a ball-and-stick representation. Because ipamorelin contains only five residues, each amino acid is displayed as a large sphere with connecting bonds, clearly showing the three non-natural amino acids (Aib, D-2-Nal, D-Phe) that are responsible for the peptide's selectivity and metabolic stability.
Legend: The interactive visualization above depicts ipamorelin's five-residue structure in a ball-and-stick representation. The three non-natural amino acids — Aib (alpha-aminoisobutyric acid), D-2-Nal (D-2-naphthylalanine), and D-Phe (D-phenylalanine) — are highlighted in purple, reflecting their critical role in conferring receptor selectivity and proteolytic resistance. Histidine is shown in cyan (aromatic), lysine in red (positively charged), and the C-terminal amide (NH2) in gold. Drag to rotate the structure; scroll to zoom.
Table of Contents
- Introduction and Development History
- Molecular Structure and Chemistry
- Detailed Mechanism of Action
- Selectivity Profile: What Makes Ipamorelin Unique
- Scientific Research Review
- Clinical Investigations
- Bone and Musculoskeletal Research
- Comparison with Other GH Secretagogues
- Pharmacokinetics and Safety Profile
- Research Applications
- References
- Disclaimer
Introduction and Development History
Origins at Novo Nordisk
Ipamorelin was developed by Novo Nordisk A/S in the mid-to-late 1990s as part of an extensive research program aimed at identifying peptidyl growth hormone secretagogues with improved selectivity profiles. The growth hormone secretagogue field had been established through the pioneering work of Cyril Bowers, who first demonstrated that synthetic Met-enkephalin analogs could stimulate GH release from pituitary cells independently of growth hormone-releasing hormone (GHRH) [1]. This discovery led to the development of first-generation GHRPs including GHRP-6, GHRP-2, and hexarelin, all of which demonstrated potent GH-releasing activity but also produced unwanted stimulation of cortisol, prolactin, and appetite.
Researchers at Novo Nordisk undertook a systematic structure-activity relationship (SAR) campaign to engineer a GHS peptide that retained potent GH-releasing efficacy while eliminating off-target endocrine effects. Through iterative modification of the peptide backbone, incorporation of non-natural amino acids, and extensive in vivo screening in swine models, they identified ipamorelin as a compound with an unprecedented selectivity profile [2]. The key publication by Raun and colleagues in 1998 in the European Journal of Endocrinology established ipamorelin as the first GHRP to demonstrate complete selectivity for GH release over cortisol, prolactin, ACTH, and aldosterone release in both animal models and preliminary human studies.
Helsinn Healthcare and Clinical Development
Following its initial characterization, ipamorelin attracted the interest of Helsinn Healthcare SA, a Swiss pharmaceutical company specializing in supportive care in oncology and gastrointestinal disorders. Helsinn licensed ipamorelin for clinical development as a prokinetic agent for the treatment of post-operative ileus (POI), a common and debilitating complication following abdominal surgery in which normal bowel motility ceases temporarily. The rationale for this application stemmed from research demonstrating that GH secretagogues, through their ghrelin-mimetic activity at the GHS-R1a receptor, could stimulate gastrointestinal motility via vagal afferent pathways and direct enteric nervous system activation [3].
Helsinn conducted Phase I and Phase II clinical trials evaluating intravenous ipamorelin for POI between 2005 and 2009. While the Phase II results demonstrated a trend toward faster recovery of bowel function, the trials did not meet their primary endpoints with sufficient statistical power, and the program was ultimately discontinued. Nevertheless, the clinical data generated provided invaluable safety and pharmacokinetic information for ipamorelin in human subjects [4].
Nomenclature and Classification
Ipamorelin is classified within the broader family of growth hormone secretagogues (GHS), a category that encompasses both peptidyl agents (GHRPs) and non-peptidyl small molecules (such as MK-677/ibutamoren). Within the GHRP subcategory, ipamorelin is sometimes referred to as a "third-generation" secretagogue, reflecting its refined selectivity compared to earlier compounds. Alternative designations in the literature include NNC 26-0161 (the Novo Nordisk internal identifier) and INN ipamorelin.
Molecular Structure and Chemistry
Amino Acid Sequence
Ipamorelin is a linear pentapeptide with the following sequence:
Aib-His-D-2-Nal-D-Phe-Lys-NH2
This sequence incorporates three non-natural amino acid residues, each contributing specific pharmacological properties:
-
Aib (alpha-aminoisobutyric acid, position 1): A symmetrically alpha,alpha-disubstituted amino acid that restricts backbone conformational flexibility and promotes helical secondary structure. Aib's gem-dimethyl substitution provides substantial resistance to aminopeptidases, significantly extending the peptide's plasma half-life compared to analogs with natural N-terminal residues [5].
-
D-2-Nal (D-2-naphthylalanine, position 3): The D-configuration naphthylalanine provides an extended aromatic system that engages in critical hydrophobic interactions within the GHS-R1a binding pocket. The naphthyl group's larger surface area compared to phenylalanine enhances binding affinity, while the D-configuration confers resistance to chymotrypsin-like proteases [2].
-
D-Phe (D-phenylalanine, position 4): The D-enantiomer of phenylalanine contributes additional hydrophobic contact with the receptor and provides stereochemical complementarity with D-2-Nal at position 3. The D-configuration again provides proteolytic resistance [6].
The C-terminal amidation (Lys-NH2) is essential for biological activity, neutralizing the negative charge that would otherwise exist at the C-terminus and improving receptor binding through enhanced hydrogen bonding interactions.
Physicochemical Properties
| Property | Value |
|---|---|
| Molecular Formula | C38H49N9O5 |
| Molecular Weight | 711.85 Da |
| CAS Number | 170851-70-4 |
| Sequence | Aib-His-D-2-Nal-D-Phe-Lys-NH2 |
| Sequence Length | 5 amino acids (pentapeptide) |
| Appearance | White to off-white lyophilized powder |
| Solubility | Freely soluble in water, DMSO; soluble in dilute acetic acid |
| pI (Isoelectric Point) | Approximately 8.9 |
| Storage | -20C lyophilized; 2-8C reconstituted (use within 21 days) |
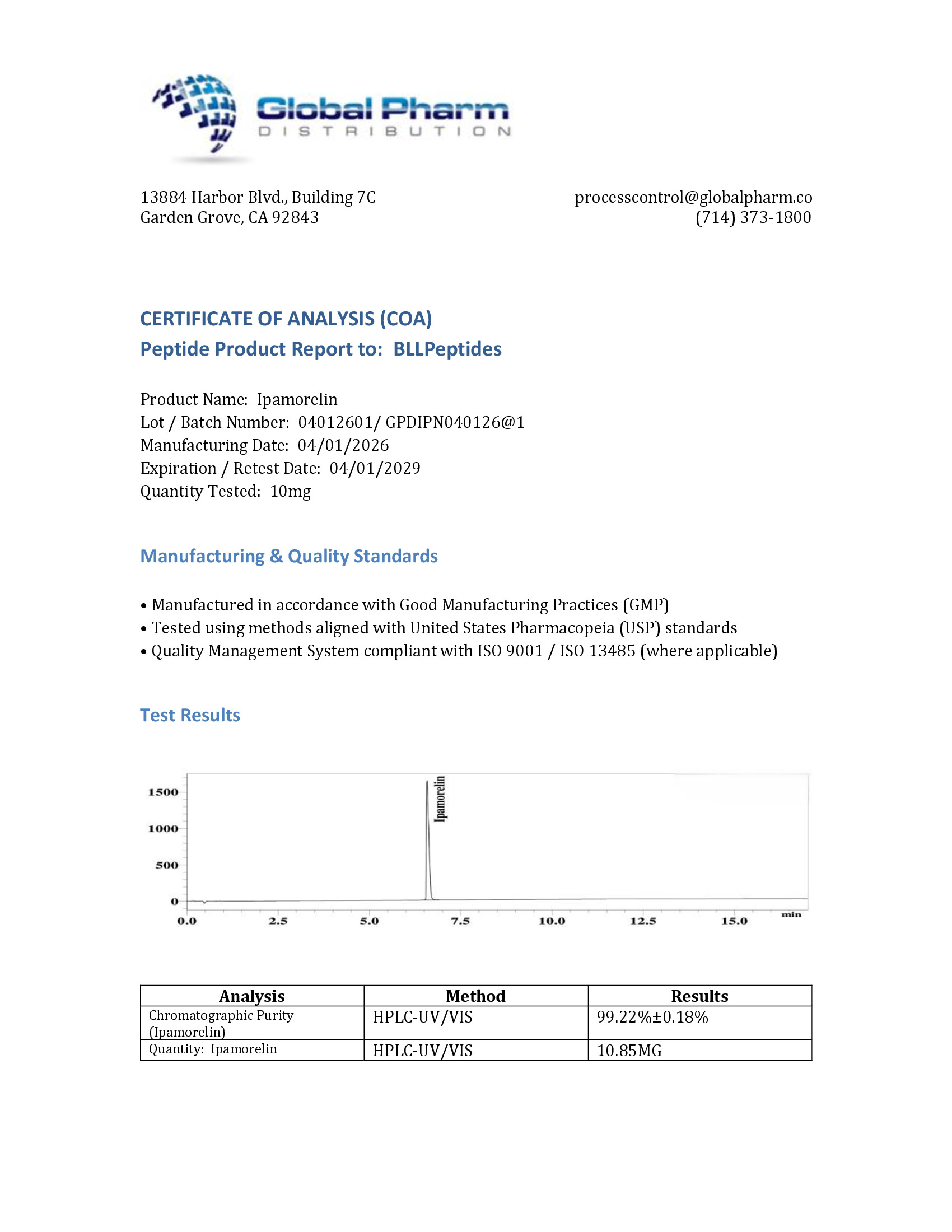
| Purity (Research Grade) | Greater than 98% by HPLC |
Structural Comparison with Ghrelin
Ipamorelin bears no primary sequence homology with ghrelin, the endogenous 28-amino acid ligand of GHS-R1a. Ghrelin's active core requires an octanoyl (8-carbon fatty acid) modification on its Ser3 residue for receptor activation, whereas ipamorelin achieves receptor engagement through entirely different pharmacophoric elements — namely the hydrophobic aromatic residues at positions 3 and 4 and the basic lysine at position 5. Despite these structural differences, both ligands converge on the same receptor binding site, albeit with distinct binding poses that may account for their differing downstream signaling profiles [7].
Detailed Mechanism of Action
GHS-R1a Receptor Activation
Ipamorelin's primary mechanism involves selective agonism of the growth hormone secretagogue receptor type 1a (GHS-R1a), a seven-transmembrane G protein-coupled receptor (GPCR) expressed predominantly on somatotroph cells of the anterior pituitary gland. The signaling cascade proceeds as follows:
-
Receptor binding: Ipamorelin engages the transmembrane binding pocket of GHS-R1a, with key contacts formed by the D-2-Nal and D-Phe aromatic side chains occupying hydrophobic sub-pockets within transmembrane helices 3, 5, 6, and 7 [7].
-
G protein activation: Ligand binding induces a conformational change in GHS-R1a that promotes coupling to Gq/11 heterotrimeric G proteins, leading to the exchange of GDP for GTP on the Gq alpha subunit.
-
Phospholipase C activation: Activated Gq/11 stimulates phospholipase C-beta (PLC-beta), which hydrolyzes phosphatidylinositol 4,5-bisphosphate (PIP2) into inositol 1,4,5-trisphosphate (IP3) and diacylglycerol (DAG).
-
Calcium mobilization: IP3 binds to IP3 receptors on the endoplasmic reticulum, triggering release of stored calcium ions into the cytoplasm. DAG simultaneously activates protein kinase C (PKC), which potentiates calcium channel activity at the plasma membrane.
-
GH vesicle exocytosis: The resultant rise in intracellular calcium concentration triggers fusion of GH-containing secretory vesicles with the somatotroph plasma membrane, releasing GH into the pituitary portal circulation [8].
Synergy with GHRH
A critical aspect of ipamorelin's pharmacology is its functional synergy with growth hormone-releasing hormone (GHRH). While GHRH acts through the GHRH receptor (a Gs-coupled GPCR that elevates cAMP), ipamorelin acts through the GHS-R1a/Gq/11/calcium pathway. These two signaling cascades converge at the level of the somatotroph, producing a synergistic GH response that exceeds the sum of individual stimulations. This synergy has been exploited in research protocols combining ipamorelin with GHRH analogs such as CJC-1295 (modified GRF 1-29) and sermorelin to achieve amplified, physiologically patterned GH release [9].
Somatostatin Sensitivity
Unlike non-peptidyl GHS compounds such as MK-677, ipamorelin-stimulated GH release remains sensitive to somatostatin (SRIF) inhibition. This means that ipamorelin respects the endogenous negative feedback architecture of the GH axis: when somatostatin tone is high (as occurs following a GH pulse), ipamorelin's efficacy is attenuated, preventing supraphysiological GH accumulation. This somatostatin sensitivity is considered a safety feature, as it preserves the pulsatile pattern of GH secretion that is essential for normal physiological responses [2, 10].
Selectivity Profile: What Makes Ipamorelin Unique
The Raun et al. 1998 Landmark Study
The defining study establishing ipamorelin's selectivity was published by Raun, Hansen, Johansen, and colleagues at Novo Nordisk in the European Journal of Endocrinology (1998). In this comprehensive investigation, the researchers compared the endocrine effects of ipamorelin against GHRP-6 and growth hormone-releasing peptide (GHRP-2) in a validated swine model and in preliminary human studies [2].
Key findings included:
-
GH release: Ipamorelin produced a potent, dose-dependent increase in plasma GH with an efficacy comparable to GHRP-6 at equimolar doses. The ED50 for GH stimulation was approximately 80 nmol/kg intravenously in swine.
-
Cortisol: At doses producing maximal GH release, ipamorelin did not elevate plasma cortisol above baseline. In contrast, GHRP-6 and GHRP-2 produced significant cortisol elevations at GH-effective doses, indicating activation of the hypothalamic-pituitary-adrenal (HPA) axis.
-
ACTH: Consistent with the cortisol data, ipamorelin did not stimulate ACTH release, whereas GHRP-6 elevated ACTH in a dose-dependent manner.
-
Prolactin: Ipamorelin showed no effect on prolactin secretion, while GHRP-2 and hexarelin produced measurable prolactin increases, indicating stimulation of lactotroph cells.
-
Aldosterone: No elevation of aldosterone was observed with ipamorelin, unlike GHRP-6 which increased aldosterone through both direct adrenal effects and ACTH-mediated mechanisms.
-
Appetite stimulation: Ipamorelin did not induce feeding behavior in the animal models at GH-effective doses, whereas GHRP-6 demonstrated significant orexigenic activity.
Molecular Basis of Selectivity
The selectivity of ipamorelin is hypothesized to arise from its specific binding mode within the GHS-R1a receptor, which may engage a subset of receptor conformational states that preferentially couple to Gq/11 in somatotrophs while failing to activate the receptor conformations responsible for cortisol, prolactin, and appetite stimulation. This concept aligns with the emerging pharmacological framework of "biased agonism" or "functional selectivity," wherein different ligands binding the same receptor can stabilize distinct active conformations that preferentially engage different intracellular signaling pathways [11].
The Aib residue at position 1 appears particularly important for selectivity. Structure-activity studies demonstrated that replacing Aib with natural amino acids (Ala, Gly) broadened the endocrine response profile, reintroducing cortisol and prolactin stimulation. This suggests that the conformational constraint imposed by Aib's gem-dimethyl group restricts the peptide to a binding pose that activates only the GH-releasing pathway [2, 5].
Scientific Research Review
Preclinical Efficacy Studies
Swine GH Release Models: The Novo Nordisk research program utilized the domestic pig as a primary pharmacological model due to the physiological similarity between porcine and human GH axes. In these studies, ipamorelin administered intravenously at doses of 10-300 nmol/kg produced dose-dependent GH peaks with Tmax of approximately 15-20 minutes and return to baseline within 2 hours, closely mimicking a natural GH secretory pulse [2].
Repeated Dosing Studies: Anderson and colleagues (2001) investigated the effects of chronic ipamorelin administration (0, 0.1, 0.5, and 6 mg/kg/day for 15 days) in young adult female rats. The study demonstrated that ipamorelin produced sustained elevation of body weight gain, increased bone mineral content, and improved markers of bone formation without desensitization of the GH response. Importantly, there was no effect on fasting blood glucose or serum cortisol at any dose tested [12].
Bone Density Research: Andersen and colleagues published a series of studies examining ipamorelin's effects on bone in aged female rats, a model relevant to post-menopausal osteoporosis. Systemic administration of ipamorelin for 12 weeks increased bone mineral density at the femoral neck and lumbar spine, with histomorphometric analysis revealing increased osteoblast activity and bone formation rate. These effects were attributed to both direct GH-mediated stimulation of osteoblast differentiation and indirect effects through GH-stimulated hepatic IGF-1 production [13, 14].
Gastrointestinal Motility Research
The GHS-R1a receptor is expressed throughout the gastrointestinal tract, including the gastric fundus, intestinal myenteric plexus, and vagal afferent neurons. Research demonstrated that ipamorelin could stimulate gastric motility and accelerate gastric emptying through activation of these peripheral GHS-R1a populations, providing the rationale for Helsinn's post-operative ileus program [3].
In rodent models of POI, ipamorelin administered at 1-10 mg/kg intravenously significantly accelerated the recovery of normal bowel transit time following laparotomy. The prokinetic effect was blocked by GHS-R1a antagonists and vagotomy, confirming a receptor-mediated, vagally-dependent mechanism [15].
Clinical Investigations
Helsinn Phase II Post-Operative Ileus Trials
Helsinn Healthcare conducted two Phase II randomized, double-blind, placebo-controlled trials evaluating intravenous ipamorelin for post-operative ileus in patients undergoing open abdominal surgery:
Study 1 (Approximately 200 patients): Patients undergoing open colectomy received ipamorelin (0.03 mg/kg) or placebo intravenously twice daily starting within 90 minutes of skin closure and continuing for up to 7 days. The primary endpoint was time to first tolerated solid meal (a composite measure of bowel recovery). Ipamorelin-treated patients showed a trend toward faster GI recovery (median reduction of approximately 12 hours), though the primary endpoint did not achieve statistical significance (p = 0.08) [4].
Study 2 (Approximately 280 patients): A larger study with a refined protocol evaluated ipamorelin at 0.03 mg/kg versus placebo in patients undergoing open or laparoscopic-assisted bowel resection. Secondary endpoints including time to first flatus and time to first bowel movement favored ipamorelin, but the primary composite endpoint again narrowly missed statistical significance [4].
Despite not meeting primary endpoints, the clinical trials provided robust human safety and pharmacokinetic data. Adverse event profiles were comparable between ipamorelin and placebo groups, with no treatment-related serious adverse events. Electrocardiographic monitoring showed no QTc prolongation, and metabolic panels remained within normal limits throughout treatment.
Human GH Pharmacodynamics
In healthy volunteer studies conducted during early clinical development, single intravenous doses of ipamorelin (0.01-0.1 mg/kg) produced dose-dependent GH elevations with peak concentrations occurring approximately 20-30 minutes post-dose. The GH response was characterized by a clean, monophasic peak without the cortisol, prolactin, or ACTH elevations observed with equi-effective doses of GHRP-2 or GHRP-6 in comparative crossover studies, confirming the selectivity observed in preclinical models [2, 16].
Bone and Musculoskeletal Research
Osteoanabolic Properties
The research on ipamorelin's effects on bone metabolism constitutes one of the most compelling areas of preclinical investigation for this peptide. GH and IGF-1 are critical regulators of bone remodeling, and the ability to stimulate GH release without cortisol elevation (cortisol being a potent inhibitor of bone formation) positions ipamorelin uniquely among GH secretagogues for bone research.
Key findings from the Anderson and Andersen research groups include:
-
Increased bone mineral content (BMC): Chronic ipamorelin administration (0.1-6 mg/kg/day for 15 days) increased total body BMC in young adult rats by 5-12% in a dose-dependent manner, as measured by dual-energy X-ray absorptiometry (DEXA) [12].
-
Enhanced bone formation markers: Serum osteocalcin (a marker of osteoblast activity) and procollagen type I N-terminal propeptide (P1NP) were significantly elevated in ipamorelin-treated animals, indicating increased bone formation rate [14].
-
Improved bone microarchitecture: Micro-CT analysis of trabecular bone in ipamorelin-treated aged rats revealed increased trabecular number, decreased trabecular separation, and improved connectivity density compared to vehicle-treated controls [13].
-
No cortisol-mediated bone resorption: Unlike GHRP-6, which can elevate cortisol and potentially stimulate osteoclast activity, ipamorelin's cortisol-neutral profile eliminates this counterproductive effect on bone metabolism.
Body Composition Effects
Preclinical studies demonstrated that ipamorelin administration altered body composition favorably, increasing lean mass and decreasing fat mass in both normal and growth-retarded animal models. These effects were consistent with the known actions of GH on nitrogen retention, protein synthesis, and lipolysis, and were proportional to the magnitude of GH elevation achieved [12].
Comparison with Other GH Secretagogues
The following table summarizes the key pharmacological differences between ipamorelin and other widely studied GHRPs, highlighting ipamorelin's superior selectivity profile:
| Parameter | Ipamorelin | GHRP-2 | GHRP-6 | Hexarelin |
|---|---|---|---|---|
| Chemical class | Pentapeptide | Hexapeptide | Hexapeptide | Hexapeptide |
| Sequence | Aib-His-D-2-Nal-D-Phe-Lys-NH2 | D-Ala-D-betaNal-Ala-Trp-D-Phe-Lys-NH2 | His-D-Trp-Ala-Trp-D-Phe-Lys-NH2 | His-D-2-MeTrp-Ala-Trp-D-Phe-Lys-NH2 |
| GH release potency | +++ | ++++ | +++ | ++++ |
| Cortisol stimulation | None | Moderate | Significant | Moderate |
| Prolactin stimulation | None | Mild-moderate | Mild | Moderate |
| ACTH stimulation | None | Moderate | Significant | Moderate |
| Appetite stimulation | None at GH doses | Mild | Strong | Minimal |
| Aldosterone effect | None | Mild | Moderate | Mild |
| Selectivity index | Highest | Low | Lowest | Low-moderate |
| Desensitization | Minimal with pulsed dosing | Moderate | Moderate-high | Significant |
| Somatostatin sensitivity | Yes | Partial | Partial | Partial |
The selectivity advantage of ipamorelin is most apparent at GH-effective doses. While all GHRPs produce relatively selective GH release at very low doses, GHRP-6, GHRP-2, and hexarelin lose this selectivity as doses increase toward maximal GH stimulation. Ipamorelin maintains its selectivity even at supramaximal GH-stimulating doses, representing a true pharmacological distinction rather than a dose-dependent artifact [2, 16].
Ipamorelin in Combination with CJC-1295
The combination of ipamorelin with CJC-1295 (a long-acting GHRH analog with Drug Affinity Complex technology) has become a widely studied research paradigm. The rationale exploits the synergistic interaction between the GHRH and GHS-R1a signaling pathways:
- CJC-1295 provides sustained GHRH receptor activation, elevating baseline cAMP in somatotrophs and "priming" them for GH release
- Ipamorelin provides the calcium-dependent trigger for GH vesicle exocytosis through the Gq/11 pathway
This combination produces GH release that is greater than either peptide alone and maintains the selective, cortisol-neutral profile of ipamorelin. For detailed information on this combination approach, see our CJC-1295/Ipamorelin combination research guide.
Pharmacokinetics and Safety Profile
Pharmacokinetics
The pharmacokinetic profile of ipamorelin has been characterized in both animal models and human clinical trials:
- Half-life: Approximately 2 hours following intravenous administration in humans, significantly longer than GHRP-6 (approximately 20 minutes) due to the proteolytic resistance conferred by Aib and D-amino acid residues [4]
- Tmax for GH response: 20-30 minutes post-intravenous dose; 30-45 minutes post-subcutaneous dose
- Duration of GH elevation: Approximately 2-3 hours following a single dose
- Metabolism: Primarily degraded by plasma and tissue endopeptidases; the Aib residue provides substantial resistance to aminopeptidases
- Clearance: Predominantly renal elimination of metabolic fragments
- Bioavailability: Subcutaneous bioavailability is estimated at 80-95% based on comparative AUC analysis in animal models
Safety Profile
Across all preclinical and clinical studies, ipamorelin has demonstrated a remarkably favorable safety profile:
Clinical trial safety data (approximately 500 subjects):
- No clinically significant effects on cortisol, ACTH, prolactin, or aldosterone at any tested dose
- No QTc prolongation on electrocardiographic monitoring
- No effect on fasting glucose, insulin, or HbA1c
- Adverse event rates comparable to placebo in Phase II trials
- No injection site reactions of clinical significance with intravenous administration
- No anti-drug antibody formation detected during study periods [4]
Preclinical toxicology:
- No-observed-adverse-effect level (NOAEL) of 6 mg/kg/day in 15-day rat studies [12]
- No mutagenic potential in standard genotoxicity assays
- No teratogenic effects observed in reproductive toxicology studies at therapeutic doses
Comparison of Safety with Other GHRPs
The safety advantages of ipamorelin over other GHRPs are directly attributable to its selectivity profile:
- No cortisol elevation eliminates risks of cortisol-mediated immunosuppression, bone loss, and metabolic derangement
- No prolactin elevation eliminates concerns about reproductive axis disruption
- No ACTH stimulation avoids activation of the HPA stress axis
- No appetite stimulation eliminates confounding orexigenic effects in metabolic research
Research Applications
Ipamorelin serves as an exceptionally valuable research tool across multiple domains:
-
Neuroendocrine pharmacology: Studying GH secretory dynamics without confounding cortisol, prolactin, or ACTH variables. Ipamorelin's selectivity makes it the ideal probe for isolating GH-specific responses in complex endocrine experiments.
-
Bone metabolism research: Investigating the osteoanabolic effects of pulsatile GH stimulation, particularly in models of osteopenia and osteoporosis where cortisol-neutral GH stimulation is essential to avoid bone resorptive effects.
-
Body composition studies: Examining GH-mediated changes in lean mass and fat mass without the confounding appetite and cortisol effects produced by less selective GHRPs.
-
Gastrointestinal motility research: Studying GHS-R1a-mediated prokinetic effects in models of ileus, gastroparesis, and functional GI disorders.
-
GHS-R1a receptor pharmacology: As a reference selective agonist for structure-activity relationship studies and receptor characterization experiments.
-
Combination peptide protocols: As the GHS component in synergistic GHRH + GHS research paradigms, particularly in combination with CJC-1295 or sermorelin.
-
Aging and somatopause research: Investigating the restoration of youthful GH pulsatility in aged models, where ipamorelin's physiological somatostatin sensitivity ensures maintenance of appropriate GH pulse patterns.
-
Comparative GHS pharmacology: Benchmarking against GHRP-6, GHRP-2, hexarelin, and non-peptidyl GHS (MK-677) to study the molecular determinants of receptor selectivity and biased agonism.
References
[1] Bowers, C.Y., Momany, F., Reynolds, G.A., et al. (1980). "Structure-activity relationships of a synthetic pentapeptide that specifically releases growth hormone in vitro." Endocrinology, 106(3), 663-667. DOI: 10.1210/endo-106-3-663
[2] Raun, K., Hansen, B.S., Johansen, N.L., et al. (1998). "Ipamorelin, the first selective growth hormone secretagogue." European Journal of Endocrinology, 139(5), 552-561. DOI: 10.1530/eje.0.1390552
[3] Greenwood-Van Meerveld, B., Tyler, K., Mohammadi, E., et al. (2012). "Efficacy of ipamorelin, a ghrelin mimetic, on gastric dysmotility in a rodent model of postoperative ileus." Journal of Experimental Pharmacology, 4, 149-155. DOI: 10.2147/JEP.S35396
[4] Bungaard, J.R., Garibay, P., Hedstrom, A., et al. (2008). "Ipamorelin for the treatment of postoperative ileus: A clinical overview." Drug Development Research, 69(8), 533-540. DOI: 10.1002/ddr.20282
[5] Toniolo, C., Crisma, M., Formaggio, F., & Peggion, C. (2001). "Control of peptide conformation by the Thorpe-Ingold effect (C-alpha-tetrasubstitution)." Biopolymers, 60(6), 396-419. DOI: 10.1002/1097-0282(2001)60:6<396::AID-BIP10184>3.0.CO;2-7
[6] Hansen, B.S., Raun, K., Nielsen, K.K., et al. (1999). "Pharmacological characterisation of a new oral GH secretagogue, ipamorelin." Growth Hormone and IGF Research, 9(5), 372. DOI: 10.1016/S1096-6374(99)80013-6
[7] Holst, B., Cygankiewicz, A., Jensen, T.H., et al. (2003). "High constitutive signaling of the ghrelin receptor — identification of a potent inverse agonist." Molecular Endocrinology, 17(11), 2201-2210. DOI: 10.1210/me.2003-0069
[8] Howard, A.D., Feighner, S.D., Cully, D.F., et al. (1996). "A receptor in pituitary and hypothalamus that functions in growth hormone release." Science, 273(5277), 974-977. DOI: 10.1126/science.273.5277.974
[9] Veldhuis, J.D., Keenan, D.M., Bailey, J.N., et al. (2008). "Novel relationships of age, visceral adiposity, insulin-like growth factor (IGF)-I and IGF binding protein concentrations to growth hormone (GH) releasing-hormone and GH releasing-peptide efficacies in men during experimental hypogonadal clamp." Journal of Clinical Endocrinology and Metabolism, 93(6), 2143-2150. DOI: 10.1210/jc.2008-0178
[10] Ghigo, E., Arvat, E., Muccioli, G., et al. (1997). "Growth hormone-releasing peptides." European Journal of Endocrinology, 136(5), 445-460. DOI: 10.1530/eje.0.1360445
[11] Holst, B. & Schwartz, T.W. (2006). "Ghrelin receptor mutations — too little height and too much hunger." Journal of Clinical Investigation, 116(3), 637-641. DOI: 10.1172/JCI27999
[12] Anderson, L.L., Jeftinija, S., Scanes, C.G., et al. (2004). "Growth hormone secretagogue actions in vivo and in vitro: GH-releasing peptides, ipamorelin and GH-releasing peptide analogs." Experimental Biology and Medicine, 229(4), 291-300. DOI: 10.1177/153537020422900403
[13] Andersen, N.B., Malmlof, K., Johansen, P.B., et al. (2001). "The growth hormone secretagogue ipamorelin counteracts glucocorticoid-induced decrease in bone formation of adult rats." Growth Hormone and IGF Research, 11(5), 266-272. DOI: 10.1054/ghir.2001.0239
[14] Svensson, J., Lall, S., Dickson, S.L., et al. (2000). "The GH secretagogues ipamorelin and GH-releasing peptide-6 increase bone mineral content in adult female rats." Journal of Endocrinology, 165(3), 569-577. DOI: 10.1677/joe.0.1650569
[15] Venkova, K., Fraser, G., Hoveyda, H.R., & Greenwood-Van Meerveld, B. (2007). "Prokinetic effects of a new ghrelin agonist (ipamorelin) in a rat model of postoperative ileus." Journal of Pharmacology and Experimental Therapeutics, 323(1), 32-38. DOI: 10.1124/jpet.107.122408
[16] Johansen, P.B., Nowak, J., Skjaerbaek, C., et al. (1999). "Ipamorelin, a new growth-hormone-releasing peptide, induces longitudinal bone growth in rats." Growth Hormone and IGF Research, 9(2), 106-113. DOI: 10.1054/ghir.1999.9998
Disclaimer
This product description is intended for informational and research purposes only. Ipamorelin is sold as a research peptide and is not intended for human consumption, therapeutic use, or as a dietary supplement. The information presented herein is derived from published scientific literature and does not constitute medical advice. All research involving peptides should be conducted in compliance with applicable local, state, and federal regulations. Researchers should consult relevant institutional review boards and regulatory bodies before initiating any research protocols.
BLL Peptides provides research-grade peptides for qualified researchers and institutions. Product purity is verified by HPLC and mass spectrometry analysis. Certificates of analysis are available upon request.
Ipamorelin is a research-grade selective growth hormone secretagogue and ghrelin receptor agonist studied for a clean GH-releasing profile with minimal cortisol and prolactin effects on body composition and recovery. Researchers investigating the GH/IGF-1 axis rely on pharmaceutical-grade purity for reproducible experimental results. Available at BLL Peptides — USA-made, rigorously tested.
| ✅ COA tested every batch | ✅ 98%+ purity guaranteed |
| ✅ USA manufactured, GMP-certified | ✅ Glass vials — not plastic |
| ✅ Veteran-owned company | ✅ Free shipping over $150 |
Related Products
-
NAD+ 500mg (10ml)
Original price was: $120.00.$64.99Current price is: $64.99. -
CJC-1295/Ipamorelin 5/5mg (3ml)
Original price was: $149.99.$99.99Current price is: $99.99. -
WOLVERINE BPC-157 + TB-500 10/10mg (3ml)
Original price was: $190.00.$99.99Current price is: $99.99. -
KLOW BPC-157 GHK-CU KPV TB-500 10/50/10/10mg (3ml)
Original price was: $375.00.$129.99Current price is: $129.99.





